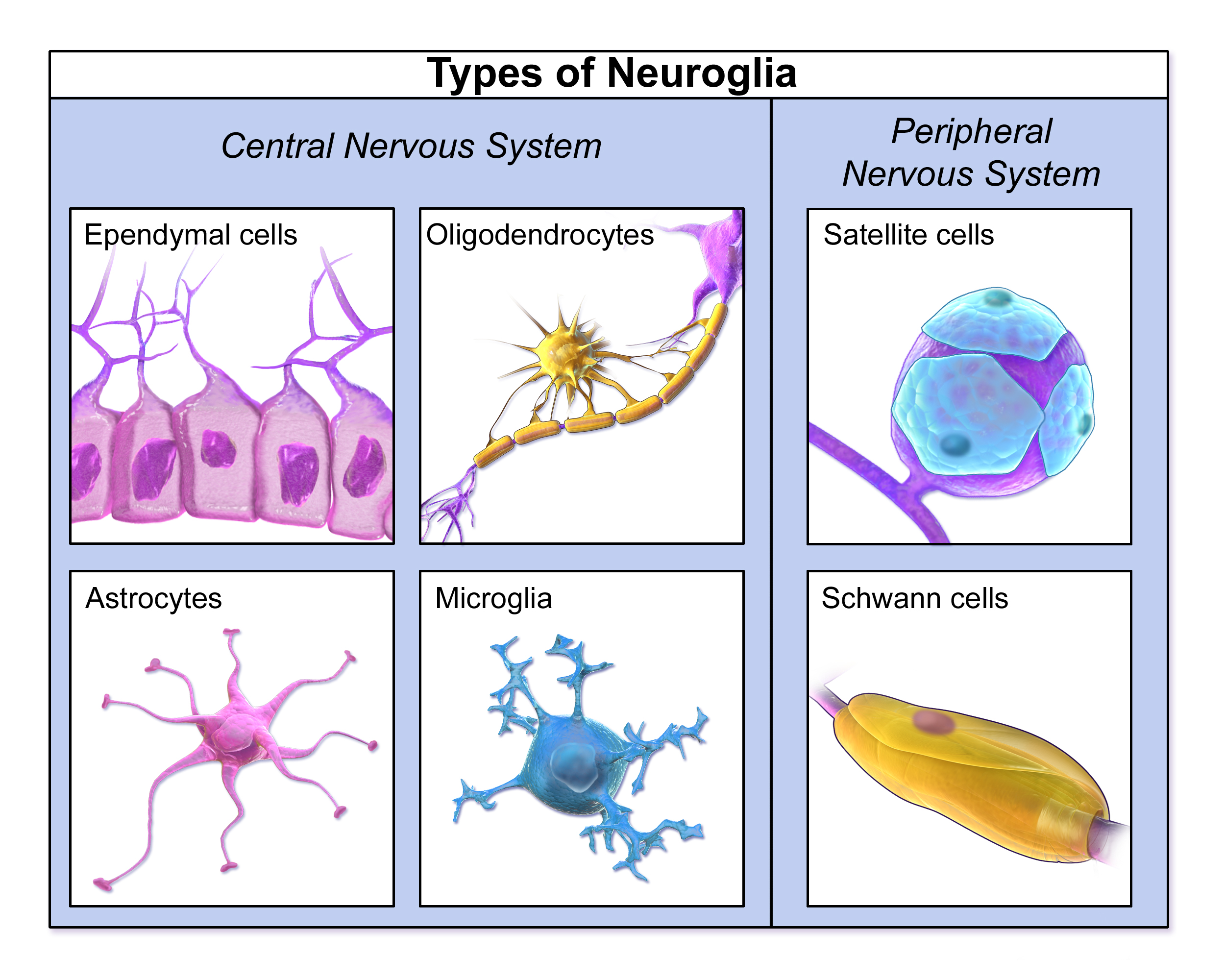
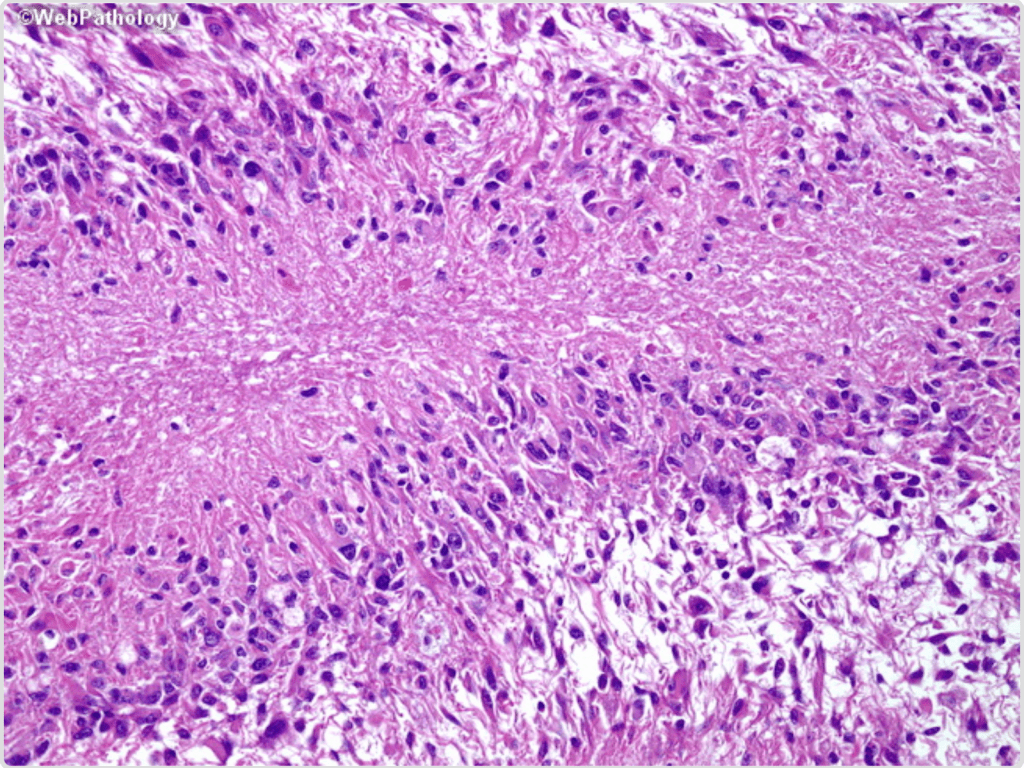
Glioblastoma (GBM) is one of the primary malignant brain tumors derived from glial cells of the central nervous system (Figure 1). Glial cells are responsible for supporting neuronal function, so one can imagine that uncontrolled growth of these cells can lead to serious neurological consequences affecting the functional processes of the brain. GBMs originate from astrocytes and masses are found within cerebral hemispheres, as a “butterfly glioma” crossing the corpus callosum (Figure 2). In histopathological slides, GBMs present as poorly differentiated primitive cells with pseudopalisading necrosis (Figure 3).
Figure 1. Major types of glial cells in the nervous system.
GBM is the most aggressive of glial tumors, as the average survival rate for patients with GBM is 14-16 months (Mohammed et al. 2022). Interestingly, there are groups of patients with GBM termed long-term survivals (LTS) that survive more than 5 years and may have distinguishing molecular, genetic, clinical, and radiographic characteristics that can be very useful for developing novel treatments for all GBM patients. The focus lies on acquiring larger LTS cohorts to make accurate predictions based on the most common characteristics these patients present. Through histological, radiological, molecular, genetic, clinical, and demographic data, researchers can develop the framework on how to identify LTS patients and develop the understanding to provide novel treatment for GBM patients.
Figure 2. Coronal T1 MRI of a typical “butterfly glioma”
Clinical findings
The most common symptoms presented in GBM patients include seizures, confusion, vision problems, facial weakness, ataxia and imbalance, memory problems and personality/behavioral changes. Although many of these symptoms can appear in LTS and short-term survivors (STS), Briceno et al. found that STS presented predominantly with seizures, headaches, and memory problems/confusion, while LTS primarily presented with difficulty in walking and uncoordinated movements. Interestingly, Briceno et al. mentioned that a relationship between STS patients and increased intracranial pressure may be a subject for further analysis. Nonetheless, definitive symptomatic clinical data is still needed. Most LTS are predominantly younger in age compared to STS.
Although this is yet to be a significant determining factor, younger age is indeed associated with longer survival rates, as these patients tend to have concurrent mutations in Isocitrate dehydrogenase (IDH), and O6 methylguanine-DNA methyltransferase (MGMT) promoter methylation, which does provide significant better survival outcomes (Wang et al. 2016). In terms of sex, Johnston et al. mention that studies that include LTS cohorts have included females predominantly. Even though GBM generally affects males more than females, larger cohorts are needed to determine if females have a protective factor that can be explained by sex. Looking further into the future, treatments are focusing on sex-specific strategies to treat patients based on their conditions.
Molecular findings
Through Next Generation Sequencing, the most common mutations found in LTS are in IDH1, IDH2 and MGMT promoter. Although IDH mutation does provide longer survival rates in GBM, it is rarely seen, and patients who had GBM with IDH mutation were no longer classified as GBM. Interestingly, molecular data found that methylation of MGMT is more commonly seen in LTS, and it may provide an underlying mechanism to study further and consider therapeutic routes involving this gene. Other molecular findings include a mutated TP53 gene, TERTp mutation, EGFR fusion, and translocation. Johnston et al. found a 17 Extreme Survival (ES) cohort study that found higher intermediate fibrillary elements and lower small anaplastic elements. Still, there is more information to be elucidated, and as genetic techniques become more sophisticated, genomic studies can be applied to treat patients with low survival probability based on distinguishing genetic characteristics found in LTS GBM patients.
Figure 3. Higher magnification showing nuclear pseudopalisading – aggregation of tumor cells around the periphery of the necrotic areas.
Imaging findings
Johnston et al. found that pre-diagnostic MRI analysis of T1 images demonstrated hypointense lesions in LTS patients, with STS presenting with mixed-intensity lesions. Gray matter involvement was mostly common in STS patients, but it is not a determinant characteristic and further imaging should be carried out. T2/FLAIR hyperintensity was more common in LTS while there were no differences in T2/FLAIR heterogeneous signals between both groups. One of the most significant results by show that contrast enhancement is significantly more prominent in wild-type IDH GBM patients. Wang et al. found that radiological features combined with IDH1 status for predicting the survival outcome of GBM patients showed that tumor contrast enhancement, multi-enhancing foci, and peritumoral edema, were found to be associated with the survival outcomes of GBM patients with IDH mutations. These findings can be used as guidelines for understanding how these tumors behave and grow.
What can Immunotherapy provide to GBM patients?
Parker et al. suggested that low clinical success to immunotherapy in GBM is due to inter and intra tumoral heterogeneity, lack of neoantigens, poor antigen presentation, and priming and secretion of immunosuppressive cytokines. External immunosuppression, low CD8 T cell activity and frequency, local T cell exhaustion and suppression, and increased frequency of immunosuppressant tumor-associated macrophages are factors that improve tumor survival chances. The need lies in developing effective immunotherapies that combat immunosuppression in GBM.
Eventually, the goal is to provide anti-tumor immunity and prolong patient survival time. The technique used to deliver the immunotherapy is via convection-enhanced delivery (CED), in which a catheter is inserted into the tumor mass to facilitate drug distribution using the positive pressure generated by the infusion pump. The process above allows the delivery of macromolecules that are too large to cross the blood-brain barrier or too toxic to be delivered systematically. Preclinical mouse glioma experiments showed that delivery via CED in mouse models leads to the killing of tumor cells and produces secondary immune responses via CD4 and CD8 T cell activation. Hopes are that clinical trials in humans can provide similar effects and use these milestones as the starting point for developing novel immunotherapy targeting tumors in all types of GBM patients.
Conclusions with some innovations in the field
Approximately 90% of GBM have poor prognosis due to the invasive and aggressive nature of this tumor. Understanding the dynamics in which glial cells develop is a key milestone for initiating strategies to treat patients with low expectations of survival. Developing novel strategies to target malignant brain tumors such as GBM is one step toward improving survival outcomes, alongside generating enough knowledge to treat other types of malignant tumors. Other advances include mathematical models to understand and predict tumor growth behavior in a personalized sex-specific manner. These unique models focus on patient-specific approaches that could potentially be more applicable to treating GBM patients in a clinical setting.
References
Mohammed, S., Dinesan, M., & Ajayakumar, T. (2022). Survival and quality of life analysis in glioblastoma multiforme with adjuvant chemoradiotherapy: a retrospective study. Reports of practical oncology and radiotherapy: journal of Greatpoland Cancer Center in Poznan and Polish Society of Radiation Oncology, 27(6), 1026–1036. https://doi.org/10.5603/RPOR.a2022.0113
Briceno, N., Vera, E., Komlodi-Pasztor, E., Abdullaev, Z., Choi, A., Grajkowska, E., Kunst, T., Levine, J., Lindsley, M., Fernandez, K., Reyes, J., Boris, L., Burton, E., Panzer, M., Polskin, L., Penas-Prado, M., Pillai, T., Theeler, B. J., Wu, J., Wall, K., … Gilbert, M. R. (2024). Long-term survivors of glioblastoma: Tumor molecular, clinical, and imaging findings. Neuro-oncology advances, 6(1), vdae019. https://doi.org/10.1093/noajnl/vdae019
Wang, K., Wang, Y., Fan, X., Wang, J., Li, G., Ma, J., Ma, J., Jiang, T., & Dai, J. (2016). Radiological features combined with IDH1 status for predicting the survival outcome of glioblastoma patients. Neuro-oncology, 18(4), 589–597. https://doi.org/10.1093/neuonc/nov239
Johnston, S. K., Whitmire, P., Massey, S. C., Kumthekar, P., Porter, A. B., Raghunand, N., Gonzalez-Cuyar, L. F., Mrugala, M. M., Hawkins-Daarud, A., Jackson, P. R., Hu, L. S., Sarkaria, J. N., Wang, L., Gatenby, R. A., Egan, K. M., Canoll, P., Swanson, K. R., & ENDURES consortium (2019). ENvironmental Dynamics Underlying Responsive Extreme Survivors (ENDURES) of Glioblastoma: A Multidisciplinary Team-based, Multifactorial Analytical Approach. American journal of clinical oncology, 42(8), 655–661. https://doi.org/10.1097/COC.0000000000000564
Parker S, McDowall C, Sanchez-Perez L, Osorio C, Duncker PC, Briley A, Swartz AM, Herndon JE 2nd, Yu YA, McLendon RE, Tedder TF, Desjardins A, Ashley DM, Gunn MD, Enterline DS, Knorr DA, Pastan IH, Nair SK, Bigner DD, Chandramohan V. Immunotoxin-αCD40 therapy activates innate and adaptive immunity and generates a durable antitumor response in glioblastoma models. Sci Transl Med. 2023 Feb 8;15(682):eabn5649. doi: 10.1126/scitranslmed.abn5649. Epub 2023 Feb 8. PMID: 36753564; PMCID: PMC10440725
Image credits:
Cover Image – Adapted from Adeberg S, Bostel T, König L, Welzel T, Debus J, Combs SE. A comparison of long-term survivors and short-term survivors with glioblastoma, subventricular zone involvement: a predictive factor for survival? Radiat Oncol. 2014 Apr 23;9:95. doi: 10.1186/1748-717X-9-95. PMID: 24758192; PMCID: PMC4011838.





[…] A. Velázquez González delves into strategies for effective brain cancer treatment in glioblastoma patients (p. […]
LikeLike